Article Text

Abstract
Objective There is limited information on the psychosocial impact of growing up with Silver-Russell syndrome (SRS), characterised by slow growth in utero leading to short stature in adulthood. Such information could aid families in making difficult treatment decisions and guide management strategies for health professionals. We aimed to explore the lived experience of people with SRS across the lifespan.
Design/setting/patients In-depth, semi-structured interviews were conducted between January 2015 and October 2016 with a sample of 15 adults (six women) with genetically confirmed SRS from the UK. Qualitative interviews were transcribed and coded to identify similarities and differences: codes were then grouped to form overarching themes.
Results Four themes were identified from participant accounts: (1) appearance-related concerns extending beyond height; (2) strategies to deal with real and perceived threats; (3) women’s experiences of pain, disability and feeling older than their years; and (4) feeling overlooked in romantic relationships. These themes show that other factors, beyond short stature, affect patient well-being and indicate a mismatch between patient need and healthcare provision.
Conclusions Challenges in SRS during childhood and adolescence were central to the psychosocial impact of SRS, and were not limited to height. These challenges, as well as symptoms such as pain and fatigue for women, have not previously been documented. To help individuals with SRS develop strategies to manage psychosocial issues, we recommend clinicians incorporate psychological services as an integral part of multidisciplinary teams managing individuals with SRS during childhood, adolescence and adulthood.
- Silver-Russell syndrome
- qualitative research
- growth
- lived experience
- psychosocial perspective
Statistics from Altmetric.com
What is already known on this topic?
The management of Silver-Russell syndrome (SRS) during childhood has a major focus on optimising height during childhood and final height.
Psychosocial evaluation is not routinely offered to children and young people in clinics.
Appearance-related concerns result in psychological distress for some individuals.
What this study adds?
Individuals with SRS have significant psychosocial concerns throughout their lives especially during childhood and adolescence.
Appearance-related concerns were not just related to height and may lead to difficulties forming romantic relationships for young people with SRS.
Pain and disability affected female participants in particular, which impacted on family relationships and employment.
Introduction
Silver-Russell syndrome (SRS) is a multisystem disorder affecting 1:30 000–100 000 children, characterised by growth failure that begins prenatally and typically leads to short stature in adulthood. Known genetic causes include errors of genomic imprinting at chromosome 11p15 and maternal uniparental disomy of chromosome 7, but 40% of clinically diagnosed cases do not demonstrate any genetic anomaly.1
Children with SRS require multidisciplinary care for problems including severe feeding difficulties, hypoglycaemia, body asymmetry2 and poor muscle function.3 Management during infancy usually focuses on feeding difficulties, prevention of hypoglycaemia and the avoidance of nutritional insufficiency. In older children, a key management goal has been to increase height during childhood and final height prognosis by optimising nutrition and administering recombinant growth hormone (GH). Individuals with SRS are typically discharged to primary care when at final height.
In short stature conditions, there has been a focus on the influence of height on psychosocial outcomes, but interpretation of findings may be complicated by the influence of associated problems. Studies of the lived experience of Turner syndrome4 5 and achondroplasia,6 7 both associated with short stature, showed adverse psychosocial issues in children and adults, including lower quality of life, depression, low self-esteem, difficulty forming relationships and social isolation. Of interest, height was not associated with quality of life scores in young women with Turner syndrome;8 and a systematic review showed that GH treatment may not ameliorate psychosocial problems.9 10
To date, psychosocial outcomes have not been studied in SRS. Childhood management focuses on height, but there are no long-term data on the outcome of this management strategy, or on the challenges faced by adults and their perceptions of health priorities. Such information will be useful to paediatricians, healthcare professionals and parents to inform management priorities for children and young people with SRS. Obtaining these data, however, is challenging given the rarity of SRS and the difficulty in identifying adults with SRS.
We undertook a qualitative research study using semi-structured in-depth interviews, with the aim to characterise the lifelong experiences of people with SRS. Qualitative research explores the meaning and complexity of a phenomenon that cannot be adequately explained numerically; a qualitative methodology is best placed to understand what it is like to live with a particular condition or to have experienced a certain phenomenon.11–13 In this study, qualitative methods were chosen to add the patient voice to the objective and clinical literature, providing a fuller picture of the lived experience of SRS, and the effect of childhood management strategies on adult outcomes.
Methods
Identification of adults with SRS
This study formed one limb of a broader study investigating the adult health consequences of SRS. Research and development approval was first gained at University Hospital Southampton NHS Foundation Trust (study sponsor) and then for the 23 UK Genetics Centres via the NIHR UK Rare Genetic Disease Research Consortium Agreement (‘Musketeers’ memorandum’). Individuals were identified across the UK using different approaches: (1) study information was disseminated through a patient support group: the Child Growth Foundation, UK; (2) individuals with SRS who had been recruited to an existing national study ‘Imprinting Disorders: finding out why’ and had expressed an interest in further research; (3) positive molecular genetics tests at the Wessex Regional Genetics Laboratory were reviewed; (4) regional genetic centres ; and (5) paediatric endocrine centres at existing genetics research sites were contacted.
Using the first two approaches, participants were sent study information by post and invited to contact the study team or were contacted by telephone if they had previously given permission. For the latter three approaches, the individual’s overseeing clinician was contacted and provided with study information to post to their patient.
Study interviews
Interviews were chosen to collect data as they allow the researcher to: focus on drawing out individual experiences; explore specific concerns or issues; be flexible about the wording of questions; and add questions about relevant topics that arise.13 As SRS is a rare condition and individuals may be known through support groups, robust confidentiality measures were instituted, including numerical participant identification and the use of age ranges (rather than specific ages). The interview schedule was constructed to address the impact of SRS on key stages in a participant’s life (education, work, friends, family, intimate relationships). Each interview took between 60 and 90 minutes and was audio recorded. A trained female researcher (LMB) experienced in discussing sensitive health issues with patients in a healthcare setting conducted the interviews. Although LMB met some participants at a clinical appointment prior to interview, it was made clear in the patient information sheet and in verbal discussions that the study was to explore what it is like to live with SRS. The study team had no preconceived ideas as to the nature of experiences participants would report.
Analysis of study interviews and thematic identification
Interviews were transcribed and analysed thematically using the well-established Braun and Clarke method.11 Tentative codes were generated from the initial transcripts and interviews were analysed as they were conducted, allowing the codes to be refined. Codes were grouped to create categories, and were developed into four overarching themes. To ensure rigour in relation to developing themes, coding and categories were independently reviewed by three researchers (LMB, AF and EJ). Tracy’s criteria were used to enhance the validity and overall quality of the study.14 NVIVO software (QSR International, V.11.3.2 (1888) for Mac) was used to manage the qualitative data.
Results
Study participants
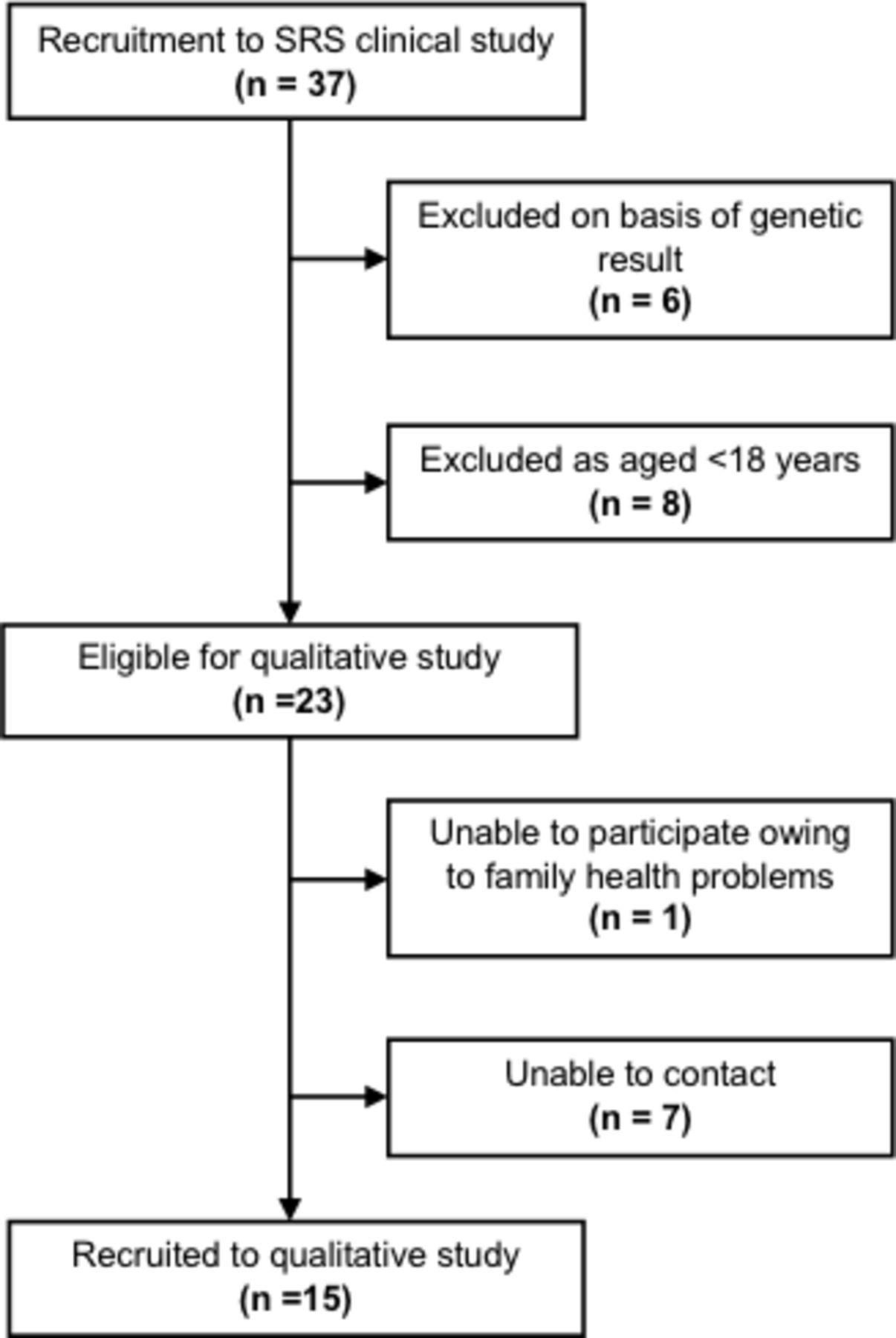
Thirty-seven adults with a molecular diagnosis of SRS were identified for the broader study, of whom 15 (six female) agreed to participate in a study interview figure 1. Of the 15 participants: 14 had a loss of methylation at 11p15 and one had maternal uniparental disomy of chromosome 7. The mean final height SD score (SDS) of this group was −2.68 (men −2.61 SDS; women −2.78 SDS) (table 1). Nine participants received GH (three female). No significant differences between participants from the broader study who did and did not participate in the qualitative study in terms of height, weight, asymmetry and molecular diagnosis were found.
Characteristics of study participants
{kind=link}
Source of recruitment to qualitative study. SRS, Silver-Russell syndrome.
Findings
Four themes were identified from participant accounts: (1) ‘it’s not just all about height’: appearance-related concerns extending beyond height; (2) resilience: strategies to deal with real and perceived threats; (3) ‘I feel like I’m an old lady’: women’s experiences of pain, disability and feeling older than their years; and (4) ‘mayor of the friend zone’: feeling overlooked in romantic relationships.
‘It’s not just all about height’: appearance-related concerns extending beyond height
At interview, 93% (n=14) of participants were employed, 80% (n=12) had a romantic partner (46% (n=7) were married), 40% (n=6) had their own families, and most appeared content with themselves and their lives: ‘I think in my thirties it has been a much more comfortable acceptance of this is who I am and kind of take it or leave it’ (P02 male). Many participants reported times when they had felt unhappy with the way they looked (table 2) and used negative words, such as ‘horrific’, ‘unattractive’, ‘ugly’ and ‘hate’ to describe how they felt about themselves. They reported concerns regarding how their appearance affected their psychological well-being, which included height but this was not the only concern raised—some participants stated that being short and asymmetrical was worse than only being short; others said that ‘it was not just about height at all’. Only two participants stated their height had impacted on their lives the most (table 3).
Examples of appearance-related concerns
Examples of characteristics participants reported they would like to change
Resilience: strategies to deal with real and perceived threats
Participants described adversities (table 4), which they perceived to be related to their diagnosis of SRS, such as: feeling different from others; discrimination; infertility; bullying; comments and staring from strangers; and negative experiences with healthcare. Strategies used by participants in response to adversity were classed as coping or adaptive strategies to reduce stress15 or cultivated resilience, for example, capitalising on other characteristics (such as humour and/or intelligence); accessing social/group support; and comparing themselves with others perceived to be less fortunate than themselves. Maladaptive ways of dealing with adversity that may have increased stress and/or psychological distress (anxiety and depression) were also identified. This included social avoidance; comparing themselves with others perceived to be more fortunate than themselves (often siblings); and not disclosing their diagnosis of SRS to others, reducing the likelihood of social support (table 5).
Adversities—quotes linked to the text regarding resilience: strategies to deal with real and perceived threats
Quotes regarding coping strategies linked to the text about resilience: strategies to deal with real and perceived threats
‘I feel like I’m an old lady’: women’s experiences of pain, disability and feeling older than their years
Female participants, especially those over 30 years, tended to depict their experience of SRS as one of pain and disability, although a few shared experiences of pain and the impact during adolescence. Some had painful joints and fatigue such that they used wheelchairs, were in receipt of disability living allowance, and some were considering modifications to their homes (stair lift). They described feeling generally ‘unwell’ and unusually tired compared with those around them. Participants felt these issues adversely affected their employment status as: they were either not employed; had to reduce their working hours as they could no longer manage; or felt they could not disclose how much their pain or disability affected them from fear of being dismissed. Participants were also concerned about the impact of their condition on their families as they had to care for them or that they were unable to attend social events due to illness or pain table 6. Only one male participant discussed experiencing pain in his neck and lower back. He attributed this to a discrepancy in leg length, which did not appear to limit his activities.
Quotes related to ‘I feel like I’m an old lady’—women’s experiences of pain, disability and feeling older than their years
‘Mayor of the friend zone’: feeling overlooked in romantic relationships
While friendships had flourished for most participants through childhood and adolescence, this was less evident for romantic relationships. One participant described being ‘mayor of the friend zone’, which has been defined as ‘an ostensibly platonic relationship in which one person is romantically interested in the other’.16 Lack of perceived romantic appeal led participants to feel they were more likely to be treated like friends by those with whom they wanted to have a romantic relationship. Although this theme was identified in the data from both male and female participants, SRS appeared to have a greater impact on male participants' romantic relationships compared with those of their peers, which for some also pervaded into adulthood. The antecedents were difficult to determine, but it is possibly related to participants' feelings of falling short regarding society’s perception of quintessentially male appearance/behaviour. This may have resulted in a subsequent lack of confidence and self-esteem. Male participants described times during adolescence and adulthood when their appearance (height and lack of muscle mass) made them feel less masculine, leading to them feeling ‘sub-standard’. Female participants described similar experiences of not fitting the ‘feminine ideal’. Some (male and female) thought they could not have relationships with people they were attracted to because they would be ‘automatically excluded’. They did not have expectations that potential romantic partners would compromise their standards to be with someone who looked like them (table 7).
Quotes in relation to ‘mayor of the friend zone’: feeling overlooked in romantic relationships
Discussion
To our knowledge, this is the first study to explore the psychosocial impact of SRS. Many individuals experienced significant adversity during childhood and adolescence relating to living with SRS, as well as physical and psychosocial issues. However, it should be noted that, at the time of interview, many participants had successful careers, were in romantic relationships, and some had, or were starting to have, families of their own.
Challenges during childhood and adolescence were central to all four themes. Participants reported starting to feel ‘different’ around aged 10 and began comparing themselves with others. They experienced bullying, staring and/or comments from strangers; and encountered problems developing romantic relationships during adolescence. Participants described disquiet regarding these issues, which were in addition to concerns about their height, and which for some led to anxiety and depression and persisted into young adulthood and beyond.
The issues experienced by participants in our study are likely to be above and beyond those experienced by young people without a health condition. Other studies have suggested that people with conditions affecting growth (idiopathic short stature, achondroplasia, Turner syndrome, constitutional growth delay) are more likely to experience psychosocial issues (lower quality of life, depression, low self-esteem, difficulty forming relationships, social isolation) compared with people within the average height range and no diagnosed health condition.4 6 17 18 Whether this is due to short stature or having a health condition, or both, is not easily understood.
While the issues experienced during adolescence were particularly problematic, young adults with SRS also experienced significant concerns at a time when specialist care ceased, when participants were facing challenging times and at a stage of life when young people experience the trials and self-doubt commonly experienced during adolescence.19 Likewise, in adults with cleft lip or palate, new issues and experiences are encountered just as the young person is discharged from paediatric services.20 Clarke et al 21 suggest transition as a good point for appearance-related concerns to be assessed, enabling health professionals (HPs) skilled in dealing with these issues to support individual needs. We would argue that for young people with SRS—and possibly other health conditions—psychosocial assessment should take place much earlier than this.
Our findings suggest that for HPs managing children and young people with SRS there needs to be greater appreciation and focus on appearance-related concerns, in addition to height, as well as psychosocial issues. A similar focus on factors other than height has improved psychosocial adjustment in children and young people with idiopathic short stature.10 It is possible that a management focus on improving height may communicate height as an aesthetic attribute, with an unhealthy focus on appearance that could contribute to appearance-related concerns beyond height. HPs also need to consider adopting a tailored approach to support, due to the gender differences in the reported experiences of individual’s SRS.
Regular psychosocial assessments are recommended for individuals with SRS.1 This is particularly pertinent as objectively rating the severity of an individual’s appearance-altering condition by HPs cannot reliably predict who will, or will not, experience psychological distress due to appearance-related concerns.22 Our findings indicate that a psychologist should be an integral member of a multidisciplinary team managing individuals with SRS during childhood, adolescence and adulthood, to aid in the development of strategies to manage any appearance-related concerns and other psychosocial issues that arise.
We have gained insight into what it is like to live with SRS through in-depth interviews, something that has not been achieved for other growth conditions. Previous research, mostly based on survey data, indicates that individuals living with short stature conditions experience a range of psychosocial issues similar to those detailed in this study.4–6 17 18 23–25 Echoing our study findings more closely, women with Turner syndrome report that height is also not their main concern;4 they had significantly more appearance and body image concerns than women without Turner syndrome,20 and experience difficulties when dating.5 8 More in-depth research is needed to explore these issues in all conditions that affect growth to ensure appropriate support is offered to children and their families. Excessive tiredness and joint pain also requires further research and long-term follow-up to understand it more fully. This may be related to the lack of muscle bulk and function in this syndrome that is often underestimated.1 It shows itself in childhood by delaying motor milestones but is subsequently not such an issue.
Our study has several limitations. We relied on participants recalling past experiences, which may have changed over time and was skewed towards a higher reporting of memories from adolescence.26 Adolescence was a crucial time when treatment and regular hospital appointments ceased, so it may be expected that adults recall more experiences from this time. Second, some participants had health conditions that may be part of, or in addition to, SRS (eg, dyslexia, cleft palate) which may lead to poor psychological adjustment.27 Teasing out which experiences were related to SRS and which were related to other health conditions was not possible, therefore we presented participants’ views on what they perceived to be related to SRS. Third, adults recalling their experiences may bear little resemblance to those of current children and young people with SRS who benefit from advancements in managing SRS. However, through speaking to young people and observing clinical appointments with children and their families, we remain confident our findings are pertinent to those actively receiving treatment. Lastly, participants were primarily those who volunteered for the broader study. These may have been a self-selecting group of individuals with complex issues, keen to have a thorough medical examination. Reflecting on the sample of participants we would say this was not the case. Participants had a range of complex health issues, with some classing themselves as ‘unaffected’ by SRS. Figure 1 shows that this substudy included all but one of the eligible participants who could be contacted, indicating a low risk of further selection bias.
The strengths of our study include several novel contributions to the field of appearance research. Our study investigated areas that are rarely reported in the literature and have not previously been described in SRS.28–33 Methodological quality in our study was enhanced by adapting the interview schedule after each interview ensuring a broad range of issues were captured. We also presented our key findings to young people and adults with SRS and their families who had not taken part in our study to triangulate our results. This gave us reassurance that the conceptual work carried out was still rooted in participants’ experiences.
Conclusion
The SRS literature to date describes the physical characteristics of SRS with little insight into living with this rare genetic condition. We have identified that individuals with SRS experience significant psychosocial issues during childhood, adolescence and adulthood which extend beyond a concern about height. These findings are relevant to paediatricians who are well positioned to anticipate and address psychosocial issues in children and young people with SRS. Such issues could be ameliorated through early psychosocial intervention; ensuring clinical appointments explore other concerns as well as growth; involving other HPs, such as psychologists and general practitioners; and by developing an adult service for individuals with SRS.
Acknowledgments
We thank the Child Growth Foundation for their support (http://www.childgrowthfoundation.org/). LMB carried out the research reported here as part of her professional doctorate in health psychology. The thesis titled ’Falling short: the psychosocial impact of living with Russell-Silver syndrome' can be found at http://ethos.bl.uk/OrderDetails.do?uin=uk.bl.ethos.714995. CDB is funded in part by the Southampton NIHR Biomedical Research Centre.
References
Footnotes
Funding This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference No PB-PG-1111-26003) with support from NIHR CRN: Wessex, NIHR Southampton BRC and NIHR Wellcome Trust Southampton Clinical Research Facility. The RfPB grant holders were IKT, JHD, JCC, CDB, AF and HI.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Competing interests JHD has received travel bursaries from Novo Nordisk, SANDOZ, Ferring and Pfizer. HI reports grants from the UK National Institute for Health Research and UK Medical Research Council (the latter for her salary) during the conduct of the study. OLS reports grants from the National Institute of Health Research during the conduct of the study.
Ethics approval NHS Research Ethics Committee South Central–Hampshire B (REC reference: 13/SC/0630).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Correction notice This paper has been amended since it was published Online First. Because of a production oversight the manuscript was published without the ‘What this study adds’ section. We have now rectified this and would like to apologise to the authors for this error.